
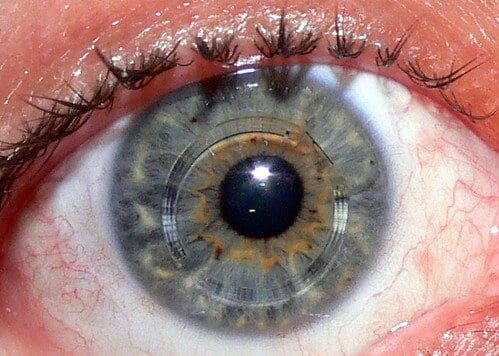
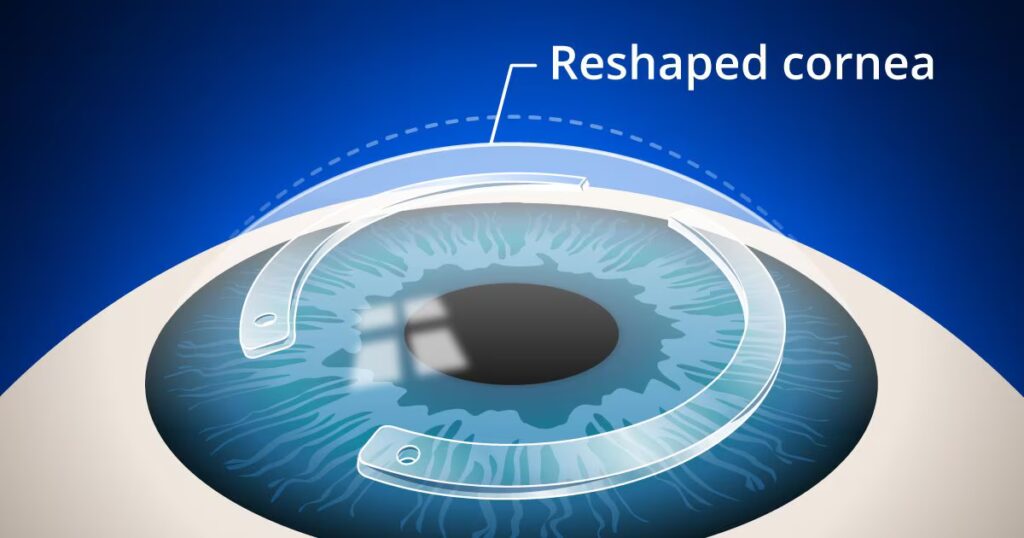
Intracorneal ring segments are small implants placed into the cornea to improve its shape in people with keratoconus. They help flatten the irregular cornea, which can improve vision and make contact lenses easier to wear.
This option is mainly for contact lens intolerant patients, often once keratoconus has stabilised or alongside CXL, and that corneal thickness is an important factor.
Types of ICRS
- Synthetic Rings (Intacs, Ferrara Rings, Keraring)
- Natural Rings (CAIRS, Kera Naturale)
Synthetic Intracorneal Ring Segments
Examples: Intacs, Ferrara Rings, Keraring
How they work:
- Made of clear plastic (PMMA).
- Reshape and regularise the cornea, reducing irregular astigmatism.
- Can improve vision, though many patients still need glasses or contact lenses.
Types of rings:
- Intacs: Placed further from the center of the cornea; generally associated with fewer side effects such as glare.
- Ferrara Rings: Placed closer to the center; often have a stronger effect on corneal reshaping, but glare or light sensitivity may be more noticeable in some patients.
Who can have them:
- Cornea must have sufficient thickness.
- No significant scarring on the cornea.
- Usually suitable for keratoconus not fully corrected with lenses.
The procedure:
- Performed under local anaesthesia.
- Quick, usually taking 15–20 minutes.
- Reversible; rings can be removed if necessary.
Long-term outcomes:
- Most rings remain in place long-term.
- Some may need removal due to glare, discomfort, or light sensitivity.
- Results vary between patients.
Choosing the Right Ring:
The best option depends on the severity and location of keratoconus, as well as the patient’s comfort and visual goals.
Natural / Allogenic Intracorneal Ring Segments
Examples: CAIRS, Kera Naturale
How they work:
- Made from donor corneal tissue rather than synthetic plastic.
- Flatten and regularise the cornea similarly to synthetic rings.
- Often combined with corneal cross-linking (CXL) to strengthen the cornea and enhance results.
Benefits:
- Biocompatible, reducing the risk of material-related complications.
- Customisable to the patient’s corneal shape.
- Reversible; can be removed if necessary.
- Minimally invasive and often suture-free, allowing faster recovery.
Who can have them:
- Typically suitable for moderate keratoconus not fully corrected with contact lenses.
- Regular follow-up is needed to monitor healing and visual outcomes.
- May not be available at all hospitals and is usually performed in specialist centres.
Outcomes:
- Can improve uncorrected distance vision and corneal shape.
- Works best when combined with CXL for both stabilisation and reshaping.
- Results vary between patients.